ب ه نام خد ا فارماکوویژیالنس و عوارض ناخواسته داروها آذر ماه 1396
|
|
|
- Jack Atkinson
- 5 years ago
- Views:
Transcription

1 ب ه نام خد ا فارماکوویژیالنس و عوارض ناخواسته داروها آذر ماه 1396


2 Upper Respiratory Tract Infections Z. Sahraei Pharm. D., Ph.D. Infectious Disease Clinical Pharmacist
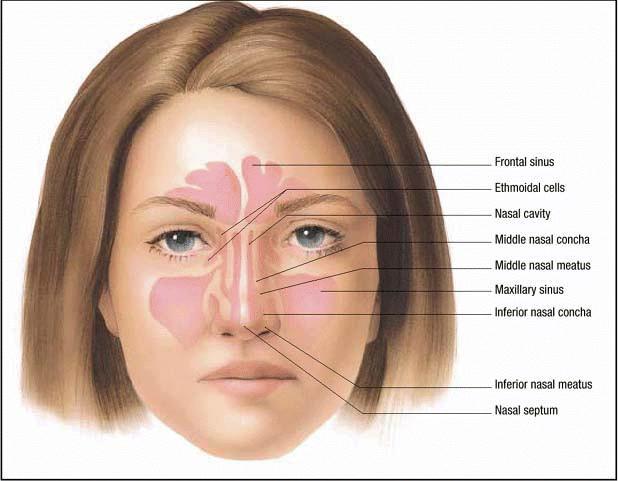
3 Rhinosinusitis
4 Definition Acute rhinosinusitis is defined as: Symptomatic inflammation of the nasal cavity and paranasal sinuses lasting up to 4 weeks. The term "rhinosinusitis" is preferred to "sinusitis" since inflammation of the sinuses rarely occurs without concurrent inflammation of the nasal mucosa.
5 Epidemiology Rhinosinusitis is an extremely common condition. Nearly 1 in 7 (13.4%) of adults aged 18 years were diagnosed with rhinosinusitis within the previous 12 months. Incidence rates among adults are higher for women than men (~1.9-fold).
6 Acute rhinosinusitis: symptoms for less than 4 weeks Subacute rhinosinusitis: symptoms for 4 to 12 weeks Chronic rhinosinusitis: persists greater than 12 weeks Recurrent acute rhinosinusitis: 4 or more episodes of ARS per year, with interim symptom resolution.
7 Etiology: Typically caused by a single pathogen. The vast majority of cases of acute rhinosinusitis (ARS) are due to viral infection (AVRS). Acute bacterial (ABRS) infection occurs in only 0.5 to 2.0 percent of episodes. The most common viruses: rhinovirus, influenza virus, and parainfluenza virus. The most common bacteria: Streptococcus pneumoniae, Haemophilus influenzae, and Moraxella catarrhalis. ABRS due to dental root infection: microaerophilic and anaerobic bacteria
8 The prevalence of a bacterial infection during acute rhinosinusitis is estimated to be 2% 10%, whereas viral causes account for 90% 98%.

9 Nasal congestion and obstruction Purulent nasal discharge Maxillary tooth discomfort Facial pain or pressure that is worse when bending forward Fever Fatigue Cough Hyposmia or anosmia Ear pressure or fullness Headache
10 Diagnosis

11 Conventional Criteria for the Diagnosis of Sinusitis Based on the Presence of at Least 2 Major or 1 Major and 2 Minor Symptoms Diagnosis of ABRS in most RCTs of antimicrobial therapy is based on the presence of compatible symptoms and signs of acute rhinosinusitis.
12 The following two criteria as most highly predictive of acute sinusitis, whether viral or bacterial: Purulent rhinorrhea Nasal congestion and facial pain/pressure Distinguishing bacterial from viral infection!!!!!!
13 IDSA ABRS Persistent symptoms or signs of ARS lasting 10 days without evidence of clinical improvement. Onset of severe symptoms or signs of high fever (>39 C) and purulent nasal discharge or facial pain for at least 3-4 consecutive days at the beginning of illness. Onset with worsening symptoms or signs: (new onset fever, headache, nasal discharge) that lasted 5-6 days and were initially improving.
14 Gold Standard The gold standard for the diagnosis of ABRS is the recovery of bacteria in high density ( 10 4 colony-forming units per milliliter) from the cavity of a paranasal sinus.

15 Imaging Studies Imaging studies such as plain radiographs or CT are frequently used by clinicians for the diagnosis of ABRS.
16 Complications Complications of ABRS: Rarely occur Related to local extension into the central nervous system and orbit of the eye.


17
18 Management of acute viral rhinosinusitis (AVRS) aims to relieve symptoms of nasal obstruction and rhinorrhea; treatment does not shorten the clinical course of the disease. Treatment for acute bacterial rhinosinusitis (ABRS) includes antibiotics to eliminate the infection and prevent complications. Studies suggest that 40 to 69 percent of patients with ABRS may clear their infection spontaneously.
19 SYMPTOMATIC THERAPY FOR ACUTE RHINOSINUSITIS Analgesics: NSAIDs and acetaminophen Topical glucocorticoids : decrease in mucosal inflammation primarily in patients with a history of allergic rhinitis Topical decongestants : no more than three consecutive days to avoid rebound congestion Oral decongestants:, pseudoephedrine, phenylephrine Antihistamines????: but over-drying of the mucosa may lead to further discomfort. Antihistamines have side effects (drowsiness), and their use for the treatment of acute sinusitis is not recommended
20 IS SALINE IRRIGATION OF THE NASAL SINUSES OF BENEfiT AS ADJUNCTIVE THERAPY IN PATIENTS WITH ABRS? Intranasal saline irrigation with either physiologic or hypertonic saline is recommended as an adjunctive treatment in adults with ABRS.
21 ANTIMICROBIALS Treatment is most often initiated empirically. Although culture-guided therapy is optimal, and is generally reserved for patients with complications.
22 Amoxicillin (500 mg three times a day) for its narrow spectrum, relatively low cost, and low sideeffect profile. Amoxicillin clavulanate is recommended as empiric therapy. The dose would be either 500 mg/125 mg orally three times daily or 875 mg/125 mg orally twice daily.
23 HIGH-DOSE AMOXICILLIN-CLAVULANATE High-dose (2 g orally BD or 90 mg/kg/day orally BD) : 1. Geographic regions with high endemic rates ( 10%) of penicillin-nonsusceptible S. pneumoniae. 2. Severe infection (evidence of systemic toxicity with fever of 39ºC or higher, and threat of suppurative complications) 3. Attendance at daycare 4. Age<2 or >65 years 5. Recent hospitalization 6. Antibiotic use within the past month 7. Immunocompromised
24 Doxycycline is a reasonable alternative for firstline therapy and can be used in patients with penicillin allergy. A respiratory fluoroquinolone (levofloxacin or moxifloxacin) is another option for penicillinallergic patients. Macrolides (clarithromycin or azithromycin), trimethoprim-sulfamethoxazole, and second- or third-generation cephalosporins are not recommended for empiric therapy because of high rates of resistance of S. pneumoniae.






")

25 SHOULD A RESPIRATORY FLUOROQUINOLONE VERSUS A B-LACTAM AGENT BE USED AS FIRST- LINE AGENTS FOR THE INITIAL EMPIRIC ANTIMICROBIAL THERAPY OF ABRS? A beta-lactam agent (amoxicillin- clavulanate) rather than a respiratory fluoroquinolone is recommended for initial empiric antimicrobial therapy of ABRS.
26 Duration for initial treatment The IDSA guidelines advise a 5 to 7 day course of antibiotics (rather than 10 to 14 days) in adults The recommended duration of therapy for uncomplicated ABRS in adults is 5 7 days. In children with ABRS, the longer treatment duration of days is still recommended.
27 INFLUENZA
28 INTRODUCTION Influenza is an acute respiratory illness caused by influenza A or B viruses that occurs in outbreaks and epidemics worldwide, mainly during the winter season. Signs and symptoms of upper and/or lower respiratory tract involvement are present, along with indications of systemic illness such as fever, headache, myalgia, and weakness. Although acutely debilitating, influenza is a self-limited infection in the general population (uncomplicated influenza); however, it is associated with increased morbidity and mortality in certain high-risk populations (complicated influenza).


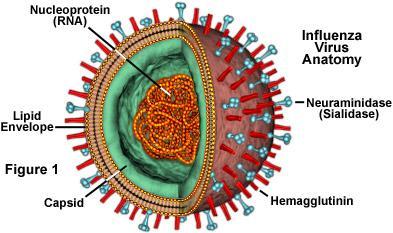
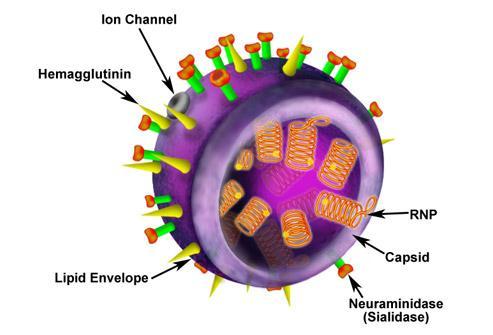
29 INFLUENZA VIRUSES A, B, AND C Influenza virus types A, B, and C are members of the Orthomyxoviridae family and affect many species, including humans, pigs, horses, and birds.
30 HEMAGGLUTININ AND NEURAMINIDASE Hemagglutinin allows the influenza virus to enter host cells by attaching to sialic acid receptors and is the major antigen to which antibodies are directed upon exposure. Neuraminidase allows the release of new viral particles from host cells by catalyzing the cleavage of linkages to sialic acid. Orthomyxovirus that contains the glycoproteins Haemagglutinin and Neuraminidase. For this reason, they are described as H1N1, H1N2 etc
31

32 PANDEMICS Spanish Flu of 1918 Asian Flu of 1957 Hong Kong Flu of 1968 Avian Influenza of 1997 Swine Flu of 2009
33 CLINICAL PRESENTATION AND DIAGNOSIS OF INFLUENZA The clinical diagnosis of influenza can be difficult because the presentation is similar to a number of other respiratory illnesses The clinical course and outcome are affected by age,immunocompetence, viral characteristics, smoking, comorbidities, pregnancy, and the degree of preexisting immunity. Complications of influenza may include exacerbation of underlying comorbidities, primary viral pneumonia, secondary bacterial pneumonia or other respiratory illnesses (e.g., sinusitis, bronchitis, otitis), encephalopathy, myocarditis, pericarditis,

34 SIGNS AND SYMPTOMS Classic signs and symptoms of influenza include rapid onset of fever, myalgia, headache, malaise, nonproductive cough, sore throat, and rhinitis. Nausea, vomiting, and otitis media are also commonly reported in children. Signs and symptoms typically resolve in approximately 3 to 7 days, although cough and malaise may persist for more than 2 weeks.
35 Complications Primary viral pneumonia: predominantly in pregnant women and in those with underlying cardiovascular disease, usually begins with fever and dry cough, which changes to a productive cough. This rapidly progresses to dyspnea, hypoxemia, and cyanosis with radiologic evidence of bilateral interstitial infiltrates. Secondary bacterial pneumonia: seen in individuals with underlying pulmonary disorders and presents during the early stages of defervescence from the influenza infection. These patients usually present with fever, productive cough, and radiologic evidence of consolidation.
36 DIAGNOSIS: LABORATORY TESTS Complete blood count and chemistry panels should be obtained to assess the overall status of the patient. The gold standard for diagnosis of influenza is viral culture, which can provide information on the specific strain and subtype. Tests such as polymerase chain reaction (RT- PCR) assay may be used for rapid detection of virus. Chest radiograph should be obtained if pneumonia is suspected.
37 GOALS OF THERAPY The four primary goals of therapy of influenza are as follows: 1. Control symptoms; 2. Prevent complications; 3. Decrease work and/or school absenteeism; 4. Prevent the spread of infection.
38 Medications Two classes of antiviral drugs are available for the treatment and prevention of influenza: The neuraminidase inhibitors, zanamivir and oseltamivir, which are active against both influenza A and B. The adamantanes, amantadine and rimantadine, which are only active against influenza A. Due to a marked increase in resistant isolates, the (ACIP) recommends that adamantanes not be used in the United States for the treatment of influenza.
39 NEURAMINIDASE INHIBITORS OSELTAMIVIR/ZANAMIVIR Oseltamivir and zanamivir are neuraminidase inhibitors that have activity against both influenza A and influenza B viruses. When administered within 48 hours of the onset of illness, oseltamivir and zanamivir may reduce the duration of illness by approximately one day versus placebo. The neuraminidase inhibitors also reduce the duration of shedding and viral titer.
40 OSELTAMIVIR TAMIFLU Prophylaxis: Oral: 75 mg once daily; initiate prophylaxis within 48 hours of contact with an infected individual; Duration of prophylaxis: 7-10 days Treatment: Oral: 75 mg twice daily initiated within 48 hours of onset of symptoms; Duration of treatment: 5 days Hospitalized patients with severe influenza infection may require longer (eg, 10 days) treatment courses Some experts have recommended empirically doubling the treatment dose (ie, 150 mg twice daily)
41 Note: Dose reduction recommended in those with creatinine clearance less than 30 ml/min. Treatment dosing of oseltamivir for children (> 7 years): 15 kg: 30 mg twice daily; 15 to 23 kg: 45 mg twice daily; 23 to 40 kg: 60 mg twice daily; >40 kg, the dose is 75 mg twice daily. The prophylactic dosing of oseltamivir for children (> 5 years ): Weight base mentioned doses once daily
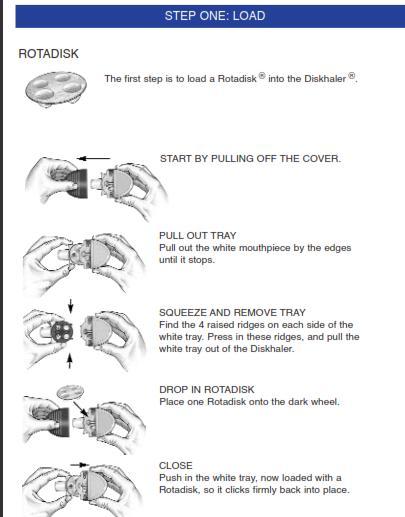
42 ZANAMIVIR - RELENZA Prophylaxis: Household setting: Two inhalations (10 mg) once daily for 10 days. Begin within 36 hours following onset of signs or symptoms of index case. Community outbreak: Two inhalations (10 mg) once daily for 28 days. Begin within 5 days of outbreak. Treatment: Two inhalations (10 mg total) twice daily for 5 days. Doses on first day should be separated by at least 2 hours; on subsequent days, doses should be spaced by ~12 hours. Begin within 2 days of signs or symptoms. Longer treatment may be considered for patients who remain severely ill after 5 days. Children (>1 year): same as adult dose

43
44 Adverse effects of neuraminidase inhibitors Zanamivir can cause bronchospasm and a decline in respiratory function in patients with asthma and other chronic respiratory disorders. As a result, the manufacturer has issued a warning advising particular caution in patients with asthma or chronic obstructive pulmonary disease. Oseltamivir can also cause nausea and vomiting, but these side effects have not generally resulted in discontinuation of therapy.
45 ADAMANTANES AMANTADINE/RIMANTADINE The adamantanes, amantadine and rimantadine, are active only against influenza A viruses, but high rates of resistance have developed and these drugs are infrequently indicated. These drugs prevent viral replication by blocking the viral M2 protein ion channel, which prevents fusion of the virus and host-cell membranes.
46 Amantadine: ACIP: Due to issues of resistance, amantadine is no longer recommended for the treatment or prophylaxis of influenza A. Influenza A treatment: Oral: 200 mg once daily or 100 mg twice daily. Initiate within hours after onset of symptoms; duration of therapy is generally 3-5 days. Influenza A prophylaxis: Oral: 200 mg once daily or 100 mg twice daily. Continue prophylaxis throughout the peak influenza activity in the community influenza season in patients who cannot be vaccinated. ADRa: CNS side effects including anxiety, insomnia, impaired thinking, confusion, lightheadedness, and hallucinations. Seizure in patients with a history of epilepsy, caution in such individuals. Anticholinergic effects that can cause dry mouth and mydriasis; as a result, it is contraindicated in patients with untreated angle closure glaucoma. These side effects appear to be related to peak drug concentrations and are more common in elderly patients
47 Rimantadine: Prophylaxis: 100 mg twice daily continue for 2 weeks and until ~10 days after illness onset in the last patient. Treatment: Oral: 100 mg twice daily ADRs: Similar CNS side effects have been described with rimantadine but at a considerably lower rate. May be associated with an increased rate of seizure activity in patients with a history of epilepsy, and should be used with caution in such individuals
48 TARGET POPULATIONS FOR TREATMENT Individuals with severe disease (requiring hospitalization or evidence of lower respiratory tract infection) Adults at high risk for complications for influenza include: 1. Residents of nursing homes and other chronic care facilities 2. Adults 65 years of age 3. Pregnant women and women up to two weeks postpartum 4. Individuals with chronic medical conditions including: Pulmonary disease, including asthma (particularly if systemic glucocorticoids have been required during the past year), Cardiovascular disease, except isolated hypertension, Active malignancy, Chronic renal insufficiency, Chronic liver disease, Diabetes mellitus, Hemoglobinopathies, such as sickle cell disease, 5. Immunosuppression, including HIV infection (particularly if CD4 <200 cells/microl), organ or hematopoietic cell transplantation, inflammatory disorders treated with immunosuppressants 6. Any neurologic condition that can compromise handling of respiratory secretions (eg, cognitive dysfunction, spinal cord injuries, seizure disorders, neuromuscular disorders) 7. Individuals who are morbidly obese (body mass index [BMI] 40)


49 Those who present >48 hours after illness onset should not be treated with antivirals since they are unlikely to benefit Patients with mild uncomplicated influenza infections who do not have risk factors for severe or complicated illness are not likely to benefit from antiviral therapy if it is initiated more than 48 hours after symptom onset
50 Oseltamivir or Zanamivir are Pregnancy Category C drugs. No adverse events have been shown to be caused by oseltamivir or zanamivir among women who received these agents during pregnancy or among infants who were exposed while in utero, although there are limited data
51 VACCINATION The primary means of influenza prevention employed in the United States is annual vaccination. Vaccination can help prevent hospitalization and death among those at high risk, decrease influenza- like illness, decrease visits to physicians offices and emergency rooms, decrease otitis media in children, and prevent school and/or work absenteeism. New vaccines are produced each year to match circulating viruses.
52 INDICATION In 2010, (ACIP) expanded the recommendation for influenza vaccination to include all individuals six months of age and older. Annual vaccination is recommended for those at high risk for complications and severe disease, such as:
53 1. 6 months through 4 years (59 months) of age 2. Are 50 years 3. Have chronic disease 4. Immunosuppressed 5. Are or will be pregnant during the influenza season 6. Are 6 months through 18 years of age and receiving long-term aspirin therapy (and may be at risk for Reye syndrome after influenza virus infection) 7. Are residents of nursing homes and other chronic-care facilities 8. Morbidly obese (body mass index [BMI] 40 for adults 9. Healthcare personnel 10. Household contacts or caregivers of children <5 years and adults 50 years of age, with particular emphasis on contacts of children <6 months 11. Household contacts or caregivers of persons with medical conditions that put them at increased risk for severe complications of influenza

54 The ideal time for vaccination is during October or November to allow for the development and maintenance of immunity during the peak of the influenza season.
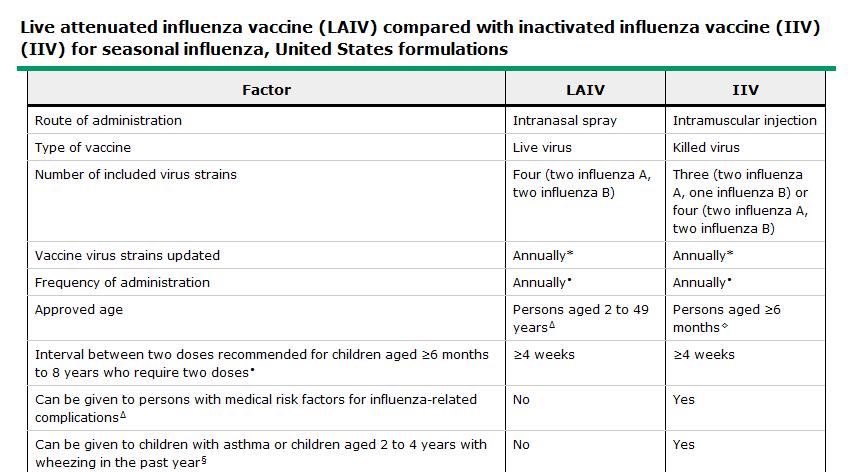
55 VACCINES TYPE In the United States, two different types of influenza vaccine are available, inactivated influenza vaccines (IIVs) and a live-attenuated vaccine (LAIV). Current influenza vaccines are trivalent or quadrivalent. The trivalent vaccine contains two influenza A virus antigens and one influenza B virus antigen, whereas the quadrivalent vaccine contains two influenza A antigens and two influenza B antigens

56 LAIV
57 PEDIATRIC VACCINATION (6 MONTH 8 YEARS) If they have never received seasonal influenza vaccine (ie, this is their first season of vaccination), or if their vaccination status cannot be determined, they should receive 2 doses separated by 4 weeks, in order to achieve satisfactory antibody response.

58

59 THE COMMON COLD
60 The most prevalent viral infection is the common cold. The frequency of the occurrence of a cold is greater in younger children and decreases with increasing age. Although the common cold is self-limiting, otitis media occurs in approximately 20% of children following infection. Many viruses have been isolated from patients with respiratory infections, but rhinovirus is the most common viral pathogen. Other pathogens include coronavirus, parainfluenza, RSV, adenovirus, and enterovirus. Because of the number of pathogens known to cause the common cold, development of an effective vaccine remains difficult.
61 TREATMENT Treatment for the common cold is directed at pharmacologic treatment of symptoms. NSAIDs, oral or intranasal decongestants, antihistamines, and antitussives may be used. However, these products provide minimal relief of symptoms and do not shorten the natural course of infection.
62 IN PEDIATRIC PATIENTS YOUNGER THAN 2 YEARS, THE USE OF COUGH AND COLD MEDICATIONS IS NOT RECOMMENDED BY THE FDA DUE TO THE DEATHS ASSOCIATED WITH THEIR USE.
63
64 PREVENTION Zinc, a dietary supplement, has been studied in both the prevention and treatment of the common cold. Echinacea is an herbal product extracted from the Echinacea plant. Echinacea is believed to stimulate the immune system, specifically phagocytosis.

65 Thank you
Upper Respiratory Tract Infections
 Upper Respiratory Tract Infections OTITIS MEDIA Otitis media is an inflammation of the middle ear. There are more than 709 million cases of otitis media worldwide each year; half of these cases occur in
Upper Respiratory Tract Infections OTITIS MEDIA Otitis media is an inflammation of the middle ear. There are more than 709 million cases of otitis media worldwide each year; half of these cases occur in
Novel H1N1 Influenza A Update. William Muth MD 2 Oct 2009
 Novel H1N1 Influenza A Update William Muth MD 2 Oct 2009 Novel H1N1 Influenza A Update Epidemiology Treatment Chemoprophylaxis Vaccine Infection Prevention Novel H1N1 Influenza A International Epidemiology
Novel H1N1 Influenza A Update William Muth MD 2 Oct 2009 Novel H1N1 Influenza A Update Epidemiology Treatment Chemoprophylaxis Vaccine Infection Prevention Novel H1N1 Influenza A International Epidemiology
THIS ACTIVITY HAS EXPIRED. CME CREDIT IS NO LONGER AVAILABLE
 THIS ACTIVITY HAS EXPIRED. CME CREDIT IS NO LONGER AVAILABLE The following content is provided for informational purposes only. PREVENTION AND CONTROL OF INFLUENZA Lisa McHugh, MPH Influenza can be a serious
THIS ACTIVITY HAS EXPIRED. CME CREDIT IS NO LONGER AVAILABLE The following content is provided for informational purposes only. PREVENTION AND CONTROL OF INFLUENZA Lisa McHugh, MPH Influenza can be a serious
Prefe f rred d t e t rm: : rhi h no n s o inu n s u iti t s
 HELP It s my sinuses! An overview of pharmacologic treatment of sinusitis Objectives Identify types of sinusitis and underlying pathology Examine common evidence based pharmacologic treatment for sinusitis
HELP It s my sinuses! An overview of pharmacologic treatment of sinusitis Objectives Identify types of sinusitis and underlying pathology Examine common evidence based pharmacologic treatment for sinusitis
Seasonal Influenza. Provider Information Sheet. Infectious Disease Epidemiology Program
 August 2007 te: This sheet contains information on seasonal influenza. For information on avian or pandemic influenza, contact the (800-423-1271 or 304-558-5358). What is influenza-like illness (ILI)?
August 2007 te: This sheet contains information on seasonal influenza. For information on avian or pandemic influenza, contact the (800-423-1271 or 304-558-5358). What is influenza-like illness (ILI)?
Novel H1N1 Influenza. It s the flu after all! William Muth M.D. Samaritan Health Services 9 November 2009
 Novel H1N1 Influenza It s the flu after all! William Muth M.D. Samaritan Health Services 9 November 2009 Influenza A Primer.. What is the flu? How do you get it? What s a virus anyhow? Can the flu be prevented,
Novel H1N1 Influenza It s the flu after all! William Muth M.D. Samaritan Health Services 9 November 2009 Influenza A Primer.. What is the flu? How do you get it? What s a virus anyhow? Can the flu be prevented,
Clinical Guidance for 2009 H1N1 Influenza and Seasonal Influenza. Barbara Wallace, MD New York State Department of Health (Updated 10/8/09)
") Clinical Guidance for 2009 H1N1 Influenza and Seasonal Influenza Barbara Wallace, MD New York State Department of Health (Updated 10/8/09) 1 Outline Clinical assessment Diagnostic testing Antiviral medications
Clinical Guidance for 2009 H1N1 Influenza and Seasonal Influenza Barbara Wallace, MD New York State Department of Health (Updated 10/8/09) 1 Outline Clinical assessment Diagnostic testing Antiviral medications
Swine Influenza Update #3. Triage, Assessment, and Care of Patients Presenting with Respiratory Symptoms
 Updated 12:00 p.m. April 30, 2009 Swine Influenza Update #3 Introduction: This document revises our last update which was sent April 28 th, 2009. The most important revisions include the following: 1.
Updated 12:00 p.m. April 30, 2009 Swine Influenza Update #3 Introduction: This document revises our last update which was sent April 28 th, 2009. The most important revisions include the following: 1.
Nothing to disclose. Influenza Update. Influenza Biology. Influenza Biology. Influenza A 12/15/2014
 Influenza Update Nothing to disclose. Lisa Winston, MD UCSF / San Francisco General Hospital Divisions of Infectious Diseases and Hospital Medicine Influenza Biology Influenza Biology Influenza viruses
Influenza Update Nothing to disclose. Lisa Winston, MD UCSF / San Francisco General Hospital Divisions of Infectious Diseases and Hospital Medicine Influenza Biology Influenza Biology Influenza viruses
Orthomyxoviridae and Paramyxoviridae. Lecture in Microbiology for medical and dental medical students
 Orthomyxoviridae and Paramyxoviridae Lecture in Microbiology for medical and dental medical students Orthomyxoviridae and Paramyxoviridae are ss RNA containng viruses Insert Table 25.1 RNA viruses 2 SIZE
Orthomyxoviridae and Paramyxoviridae Lecture in Microbiology for medical and dental medical students Orthomyxoviridae and Paramyxoviridae are ss RNA containng viruses Insert Table 25.1 RNA viruses 2 SIZE
Respiratory System Virology
 Respiratory System Virology Common Cold: Rhinitis. A benign self limited syndrome caused by several families of viruses. The most frequent acute illness in industrialized world. Mild URT illness involving:
Respiratory System Virology Common Cold: Rhinitis. A benign self limited syndrome caused by several families of viruses. The most frequent acute illness in industrialized world. Mild URT illness involving:
Q: If antibody to the NA and HA are protective, why do we continually get epidemics & pandemics of flu?
 Influenza virus Influenza virus Orthomyxoviridae family of viruses RNA enveloped viruses that make up three genera Influenzavirus A Influenzavirus B Influenzavirus C The type A viruses are the most virulent
Influenza virus Influenza virus Orthomyxoviridae family of viruses RNA enveloped viruses that make up three genera Influenzavirus A Influenzavirus B Influenzavirus C The type A viruses are the most virulent
Influenza A 6/23/2010. Lisa Winston, MD UCSF / San Francisco General Hospital Divisions of Infectious Diseases and Hospital Medicine
 Influenza Update in a Pandemic Year Nothing to disclose. Lisa Winston, MD UCSF / San Francisco General Hospital Divisions of Infectious Diseases and Hospital Medicine Influenza Biology Influenza Biology
Influenza Update in a Pandemic Year Nothing to disclose. Lisa Winston, MD UCSF / San Francisco General Hospital Divisions of Infectious Diseases and Hospital Medicine Influenza Biology Influenza Biology
PEDIATRIC INFLUENZA CLINICAL PRACTICE GUIDELINES
 PEDIATRIC INFLUENZA CLINICAL PRACTICE GUIDELINES DEFINITIONS AND BACKGROUND Uncomplicated influenza illness is characterized by the abrupt onset of constitutional and respiratory signs and symptoms. Signs
PEDIATRIC INFLUENZA CLINICAL PRACTICE GUIDELINES DEFINITIONS AND BACKGROUND Uncomplicated influenza illness is characterized by the abrupt onset of constitutional and respiratory signs and symptoms. Signs
continuing education for pharmacists
 continuing education for pharmacists Common Cold, Sinusitis, Influenza: The Diseases, Prevention, Treatment Volume XXX, No. 11 Mona T. Thompson, R.Ph., PharmD Dr. Mona T. Thompson has no relevant financial
continuing education for pharmacists Common Cold, Sinusitis, Influenza: The Diseases, Prevention, Treatment Volume XXX, No. 11 Mona T. Thompson, R.Ph., PharmD Dr. Mona T. Thompson has no relevant financial
COUNTY OF MORRIS DEPARTMENT OF LAW & PUBLIC SAFETY OFFICE OF HEALTH MANAGEMENT
 1 COUNTY OF MORRIS DEPARTMENT OF LAW & PUBLIC SAFETY OFFICE OF HEALTH MANAGEMENT P.O. Box 900 Morristown, NJ 07963 (973) 631-5485 (973) 631-5490 Fax www.morrishealth.org 2012-2013 Influenza Season FREQUENTLY
1 COUNTY OF MORRIS DEPARTMENT OF LAW & PUBLIC SAFETY OFFICE OF HEALTH MANAGEMENT P.O. Box 900 Morristown, NJ 07963 (973) 631-5485 (973) 631-5490 Fax www.morrishealth.org 2012-2013 Influenza Season FREQUENTLY
Tamiflu. Tamiflu (oseltamivir) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.01.19 Subject: Tamiflu Page: 1 of 5 Last Review Date: March 18, 2016 Tamiflu Description Tamiflu (oseltamivir)
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.01.19 Subject: Tamiflu Page: 1 of 5 Last Review Date: March 18, 2016 Tamiflu Description Tamiflu (oseltamivir)
INFLUENZA VIRUS. INFLUENZA VIRUS CDC WEBSITE
 INFLUENZA VIRUS INFLUENZA VIRUS CDC WEBSITE http://www.cdc.gov/ncidod/diseases/flu/fluinfo.htm 1 THE IMPACT OF INFLUENZA Deaths: PANDEMICS 1918-19 S p a n is h flu 5 0 0,0 0 0 U S 2 0,0 0 0,0 0 0 w o rld
INFLUENZA VIRUS INFLUENZA VIRUS CDC WEBSITE http://www.cdc.gov/ncidod/diseases/flu/fluinfo.htm 1 THE IMPACT OF INFLUENZA Deaths: PANDEMICS 1918-19 S p a n is h flu 5 0 0,0 0 0 U S 2 0,0 0 0,0 0 0 w o rld
Current Trend in URTI
 Current Trend in URTI Dr Chow Chun Kuen Specialist in Otorhinolaryngology Upper respiratory tract infection Nonspecific Most common cause of physician visits & sick leaves Acute infection of noes, sinuses,
Current Trend in URTI Dr Chow Chun Kuen Specialist in Otorhinolaryngology Upper respiratory tract infection Nonspecific Most common cause of physician visits & sick leaves Acute infection of noes, sinuses,
Sinusitis in Adults UP TO DATE
 Sinusitis in Adults UP TO DATE Acute sinusitis and rhinosinusitis in adults: Treatment Authors Peter H Hwang, MD Anne Getz, MD Section Editors Daniel G Deschler, MD, FACS Stephen B Calderwood, MD Deputy
Sinusitis in Adults UP TO DATE Acute sinusitis and rhinosinusitis in adults: Treatment Authors Peter H Hwang, MD Anne Getz, MD Section Editors Daniel G Deschler, MD, FACS Stephen B Calderwood, MD Deputy
PUBLIC HEALTH SIGNIFICANCE SEASONAL INFLUENZA AVIAN INFLUENZA SWINE INFLUENZA
 INFLUENZA DEFINITION Influenza is an acute highly infectious viral disease characterized by fever, general and respiratory tract catarrhal manifestations. Influenza has 3 Types Seasonal Influenza Avian
INFLUENZA DEFINITION Influenza is an acute highly infectious viral disease characterized by fever, general and respiratory tract catarrhal manifestations. Influenza has 3 Types Seasonal Influenza Avian
A Just in Time Primer on H1N1 Influenza A and Pandemic Influenza developed by the National Association of State EMS Officials and Revised by the
 A Just in Time Primer on H1N1 Influenza A and Pandemic Influenza developed by the National Association of State EMS Officials and Revised by the Michigan Department of Community Health EMS and Trauma Systems
A Just in Time Primer on H1N1 Influenza A and Pandemic Influenza developed by the National Association of State EMS Officials and Revised by the Michigan Department of Community Health EMS and Trauma Systems
Diagnosing and managing
 www.bpac.org.nz keyword: influenza influenza Diagnosing and managing Key reviewers: Associate Professor Mark Thomas, Infectious Disease Specialist, School of Medical Sciences, University of Auckland Dr
www.bpac.org.nz keyword: influenza influenza Diagnosing and managing Key reviewers: Associate Professor Mark Thomas, Infectious Disease Specialist, School of Medical Sciences, University of Auckland Dr
2009 (Pandemic) H1N1 Influenza Virus
 H1N1 Influenza Virus") 2009 (Pandemic) H1N1 Influenza Virus September 15, 2009 Olympia, Washington Anthony A Marfin Washington State Department of Health Goals Understand current situation & pattern of transmission of 2009 H1N1
2009 (Pandemic) H1N1 Influenza Virus September 15, 2009 Olympia, Washington Anthony A Marfin Washington State Department of Health Goals Understand current situation & pattern of transmission of 2009 H1N1
Influenza Outbreaks. An Overview for Pharmacists Prescribing Antiviral Medications
 Influenza Outbreaks An Overview for Pharmacists Prescribing Antiviral Medications Under the Collaborative Drug Therapy Agreement for Influenza Antiviral Medications Learning Objectives 1. Understand the
Influenza Outbreaks An Overview for Pharmacists Prescribing Antiviral Medications Under the Collaborative Drug Therapy Agreement for Influenza Antiviral Medications Learning Objectives 1. Understand the
Pandemic H1N1 2009: The Public Health Perspective. Massachusetts Department of Public Health November, 2009
 Pandemic H1N1 2009: The Public Health Perspective Massachusetts Department of Public Health November, 2009 Training Objectives Describe and distinguish between seasonal and pandemic influenza. Provide
Pandemic H1N1 2009: The Public Health Perspective Massachusetts Department of Public Health November, 2009 Training Objectives Describe and distinguish between seasonal and pandemic influenza. Provide
Acute respiratory illness This is a disease that typically affects the airways in the nose and throat (the upper respiratory tract).
.") Influenza glossary Adapted from the Centers for Disease Control and Prevention, US https://www.cdc.gov/flu/glossary/index.htm and the World Health Organization http://www.wpro.who.int/emerging_diseases/glossary_rev_sept28.pdf?ua=1
Influenza glossary Adapted from the Centers for Disease Control and Prevention, US https://www.cdc.gov/flu/glossary/index.htm and the World Health Organization http://www.wpro.who.int/emerging_diseases/glossary_rev_sept28.pdf?ua=1
The pages that follow contain information critical to protecting the health of your patients and the citizens of Colorado.
 Health Alert Network Tri-County Health Department Serving Adams, Arapahoe and Douglas Counties Phone 303/220-9200 Fax 303/741-4173 www.tchd.org Follow us on Twitter @TCHDHealth and @TCHDEmergency John
Health Alert Network Tri-County Health Department Serving Adams, Arapahoe and Douglas Counties Phone 303/220-9200 Fax 303/741-4173 www.tchd.org Follow us on Twitter @TCHDHealth and @TCHDEmergency John
NEW YORK CITY DEPARTMENT OF HEALTH AND MENTAL HYGIENE Thomas R. Frieden, MD, MPH Commissioner
 NEW YORK CITY DEPARTMENT OF HEALTH AND MENTAL HYGIENE Thomas R. Frieden, MD, MPH Commissioner Interim Guidance on Dosage, Precautions, and Adverse Effects of Antiviral Medications used to Treat or Prevent
NEW YORK CITY DEPARTMENT OF HEALTH AND MENTAL HYGIENE Thomas R. Frieden, MD, MPH Commissioner Interim Guidance on Dosage, Precautions, and Adverse Effects of Antiviral Medications used to Treat or Prevent
Rhinosinusitis. John Ramey, MD Joseph Russell, MD
 Rhinosinusitis John Ramey, MD Joseph Russell, MD Disclosure Statement RSFH as a continuing medical education provider, accredited by the South Carolina Medical Association, it is the policy of RSFH to
Rhinosinusitis John Ramey, MD Joseph Russell, MD Disclosure Statement RSFH as a continuing medical education provider, accredited by the South Carolina Medical Association, it is the policy of RSFH to
UPPER RESPIRATORY TRACT INFECTIONS. IAP UG Teaching slides
 UPPER RESPIRATORY TRACT INFECTIONS 1 INTRODUCTION Most common problem in children below 5 years. In this age group they get about 6 8 episodes per year. It includes infections of nasal cavity, throat,
UPPER RESPIRATORY TRACT INFECTIONS 1 INTRODUCTION Most common problem in children below 5 years. In this age group they get about 6 8 episodes per year. It includes infections of nasal cavity, throat,
Influenza B viruses are not divided into subtypes, but can be further broken down into different strains.
 Influenza General Information Influenza (the flu) is a highly transmissible respiratory illness caused by influenza viruses. It can cause mild to severe illness, and may lead to death. Older people, young
Influenza General Information Influenza (the flu) is a highly transmissible respiratory illness caused by influenza viruses. It can cause mild to severe illness, and may lead to death. Older people, young
Influenza: Questions and Answers
 Influenza: Questions and Answers Information about the disease and vaccines What causes influenza? Viruses cause influenza. There are two basic types, A and B. Their genetic material differentiates them.
Influenza: Questions and Answers Information about the disease and vaccines What causes influenza? Viruses cause influenza. There are two basic types, A and B. Their genetic material differentiates them.
Influenza RN.ORG, S.A., RN.ORG, LLC
 Influenza WWW.RN.ORG Reviewed May, 2017, Expires May, 2019 Provider Information and Specifics available on our Website Unauthorized Distribution Prohibited 2017 RN.ORG, S.A., RN.ORG, LLC PURPOSE: This
Influenza WWW.RN.ORG Reviewed May, 2017, Expires May, 2019 Provider Information and Specifics available on our Website Unauthorized Distribution Prohibited 2017 RN.ORG, S.A., RN.ORG, LLC PURPOSE: This
Influenza in the pediatric population
 Influenza in the pediatric population Annual attack rates 10%-40% in children Hospitalization Increased risk in children
Influenza in the pediatric population Annual attack rates 10%-40% in children Hospitalization Increased risk in children
Update I had a little bird, It s name was Enza, I opened up the window, And In Flu Enza.
 I had a little bird, It s name was Enza, I opened up the window, And In Flu Enza. Update 2014 2015 Timothy R. Cassity, Ph.D. Microbiologist Southern Ohio Medical Center January 16, 2015 The opinions expressed
I had a little bird, It s name was Enza, I opened up the window, And In Flu Enza. Update 2014 2015 Timothy R. Cassity, Ph.D. Microbiologist Southern Ohio Medical Center January 16, 2015 The opinions expressed
Revised Recommendations for the Use of Influenza Antiviral Drugs
 QUESTIONS & ANSWERS Revised Recommendations for the Use of Influenza Antiviral Drugs Background On September 8, 2009 CDC updated its recommendations for the use of influenza antiviral medicines to provide
QUESTIONS & ANSWERS Revised Recommendations for the Use of Influenza Antiviral Drugs Background On September 8, 2009 CDC updated its recommendations for the use of influenza antiviral medicines to provide
Influenza: The past, the present, the (future) pandemic
 pandemic") Influenza: The past, the present, the (future) pandemic Kristin Butler, MLS (ASCP) cm Department of Clinical Laboratory Sciences Louisiana Health Sciences Center - Shreveport Fall 2017 Objectives 1) Detail
Influenza: The past, the present, the (future) pandemic Kristin Butler, MLS (ASCP) cm Department of Clinical Laboratory Sciences Louisiana Health Sciences Center - Shreveport Fall 2017 Objectives 1) Detail
1/31/2013 DISEASE BASICS. Influenza; Implications for Public Health Professionals. Influenza: An Age-Old Disease, A Disease for All Ages
 Influenza; Implications for Public Health Professionals Phillip L. Barkley, M.D. Director of Student Health University of Florida DISEASE BASICS Influenza: An Age-Old Disease, A Disease for All Ages Epidemics
Influenza; Implications for Public Health Professionals Phillip L. Barkley, M.D. Director of Student Health University of Florida DISEASE BASICS Influenza: An Age-Old Disease, A Disease for All Ages Epidemics
Respiratory Viruses. Respiratory Syncytial Virus
 Adam Ratner, MD Respiratory Viruses Respiratory viruses are among the most common causes of disease throughout life. Often mild and self-limited, they are still associated with tremendous economic and
Adam Ratner, MD Respiratory Viruses Respiratory viruses are among the most common causes of disease throughout life. Often mild and self-limited, they are still associated with tremendous economic and
High dose amoxicillin for sinusitis
 High dose amoxicillin for sinusitis Amoxil ( amoxicillin ) is a commonly used penicillin antibiotic. It is produced in tablets (500 mg 875 mg), capsules, chewable tablets and oral suspensions. 6-3-2018
High dose amoxicillin for sinusitis Amoxil ( amoxicillin ) is a commonly used penicillin antibiotic. It is produced in tablets (500 mg 875 mg), capsules, chewable tablets and oral suspensions. 6-3-2018
Influenza Exposure Medical Response Guidance for the University of Wisconsin-Madison
 Influenza Exposure Medical Response Guidance for the University of Wisconsin-Madison 1.0 Instructions: Information in this guidance is meant to inform both laboratory staff and health professionals about
Influenza Exposure Medical Response Guidance for the University of Wisconsin-Madison 1.0 Instructions: Information in this guidance is meant to inform both laboratory staff and health professionals about
Update on Rhinosinusitis 2013 AAP Guidelines Review
 Update on Rhinosinusitis 2013 AAP Guidelines Review Carla M. Giannoni, MD Surgeon, Otolaryngology Texas Children's Hospital Professor, Surgery and Pediatrics, Baylor College of Medicine CDC: Acute Rhinosinusitis
Update on Rhinosinusitis 2013 AAP Guidelines Review Carla M. Giannoni, MD Surgeon, Otolaryngology Texas Children's Hospital Professor, Surgery and Pediatrics, Baylor College of Medicine CDC: Acute Rhinosinusitis
Influenza. Paul K. S. Chan Department of Microbiology The Chinese University of Hong Kong
 Influenza Paul K. S. Chan Department of Microbiology The Chinese University of Hong Kong Influenza Virus Nomenclature Influenza virus A, B & C Influenza A : Haemagglutinin (H), neuraminidase (N) A H3N2,
Influenza Paul K. S. Chan Department of Microbiology The Chinese University of Hong Kong Influenza Virus Nomenclature Influenza virus A, B & C Influenza A : Haemagglutinin (H), neuraminidase (N) A H3N2,
HEALTH ALERT SWINE INFLUENZA SITUATION UPDATE UPDATED PATIENT TESTING PRIORITIZATION INTERIM GUIDANCE ON ANTIVIRALS
 HEALTH ALERT SWINE INFLUENZA SITUATION UPDATE UPDATED PATIENT TESTING PRIORITIZATION INTERIM GUIDANCE ON ANTIVIRALS DATE: May 7, 2009 TO: Physicians, Providers, and Pharmacists in San Joaquin County FROM:
HEALTH ALERT SWINE INFLUENZA SITUATION UPDATE UPDATED PATIENT TESTING PRIORITIZATION INTERIM GUIDANCE ON ANTIVIRALS DATE: May 7, 2009 TO: Physicians, Providers, and Pharmacists in San Joaquin County FROM:
Acute Otitis Media, Acute Bacterial Sinusitis, and Acute Bacterial Rhinosinusitis
 Acute Otitis Media, Acute Bacterial Sinusitis, and Acute Bacterial Rhinosinusitis This guideline, developed by Larry Simmons, MD, in collaboration with the ANGELS team, on October 3, 2013, is a significantly
Acute Otitis Media, Acute Bacterial Sinusitis, and Acute Bacterial Rhinosinusitis This guideline, developed by Larry Simmons, MD, in collaboration with the ANGELS team, on October 3, 2013, is a significantly
Prevention and Treatment of Seasonal Influenza. What to expect. Objectives 11/5/14
 Prevention and Treatment of Seasonal Influenza Jason M. Pogue, PharmD, BCPS-ID Clinical Pharmacist, Infectious Diseases Sinai-Grace Hospital; Detroit Medical Center 7 November 2014 What to expect http://www.michigan.gov/mdch
Prevention and Treatment of Seasonal Influenza Jason M. Pogue, PharmD, BCPS-ID Clinical Pharmacist, Infectious Diseases Sinai-Grace Hospital; Detroit Medical Center 7 November 2014 What to expect http://www.michigan.gov/mdch
Diagnosis of Seasonal and Pandemic Influenza. Objectives. Influenza Infections 11/7/2014
 Diagnosis of Seasonal and Pandemic Influenza Michael Klepser, Pharm.D., FCCP Professor Ferris State University College of Pharmacy Objectives Given a patient case, be able to identify signs and symptoms
Diagnosis of Seasonal and Pandemic Influenza Michael Klepser, Pharm.D., FCCP Professor Ferris State University College of Pharmacy Objectives Given a patient case, be able to identify signs and symptoms
INFLUENZA VACCINATION AND MANAGEMENT SUMMARY
 INFLUENZA VACCINATION AND MANAGEMENT SUMMARY Morbidity and mortality related to influenza occur at a higher rate in people over 65 and those with underlying chronic medical conditions. Annual influenza
INFLUENZA VACCINATION AND MANAGEMENT SUMMARY Morbidity and mortality related to influenza occur at a higher rate in people over 65 and those with underlying chronic medical conditions. Annual influenza
Swine Flu; Symptoms, Precautions & Treatments
 Swine Flu; Symptoms, Precautions & Treatments What is the swine flu? Swine flu, also known as the H1N1 virus, is a relatively new strain of an influenza virus that causes symptoms similar to the regular
Swine Flu; Symptoms, Precautions & Treatments What is the swine flu? Swine flu, also known as the H1N1 virus, is a relatively new strain of an influenza virus that causes symptoms similar to the regular
RESPIRATORY TRACT INFECTIONS. CLS 212: Medical Microbiology Zeina Alkudmani
 RESPIRATORY TRACT INFECTIONS CLS 212: Medical Microbiology Zeina Alkudmani Lower Respiratory Tract Upper Respiratory Tract Anatomy of the Respiratory System Nasopharynx Oropharynx Respiratory Tract Infections
RESPIRATORY TRACT INFECTIONS CLS 212: Medical Microbiology Zeina Alkudmani Lower Respiratory Tract Upper Respiratory Tract Anatomy of the Respiratory System Nasopharynx Oropharynx Respiratory Tract Infections
Treatment of Influenza. Dr. YU Wai Cho
 Treatment of Influenza Dr. YU Wai Cho Symptomatic Treatment Analgesics/ Antipyretics (avoid aspirin) Adequate fluids Rest Specific Drug Treatment Synthetic amines Amantadine Rimantadine Neuraminidase inhibitors
Treatment of Influenza Dr. YU Wai Cho Symptomatic Treatment Analgesics/ Antipyretics (avoid aspirin) Adequate fluids Rest Specific Drug Treatment Synthetic amines Amantadine Rimantadine Neuraminidase inhibitors
Infant and Pediatric Influenza. Mike Czervinske RRT-NPS University of Kansas Medical Center
 Infant and Pediatric Influenza Mike Czervinske RRT-NPS University of Kansas Medical Center Influenza Infants and Influenza Acute infection of the respiratory tract Nose Throat Possibly lungs Pathophysiology
Infant and Pediatric Influenza Mike Czervinske RRT-NPS University of Kansas Medical Center Influenza Infants and Influenza Acute infection of the respiratory tract Nose Throat Possibly lungs Pathophysiology
ESCMID Online Lecture Library. by author
 INFLUENZA IN CHILDREN Cristian Launes Infectious Diseases Unit. Department of Paediatrics. Hospital Sant Joan de Déu (Universitat de Barcelona) Innovation in Severe Acute Respiratory Infections (SARI),
INFLUENZA IN CHILDREN Cristian Launes Infectious Diseases Unit. Department of Paediatrics. Hospital Sant Joan de Déu (Universitat de Barcelona) Innovation in Severe Acute Respiratory Infections (SARI),
Upper Respiratory Tract Infections / 42
 Upper Respiratory Tract Infections 1 Upper Respiratory Tract Infections Acute tonsillitispharyngitis Acute otitis media Acute sinusitis Common cold Acute laryngitis Otitis externa Mastoiditis Acute apiglottis
Upper Respiratory Tract Infections 1 Upper Respiratory Tract Infections Acute tonsillitispharyngitis Acute otitis media Acute sinusitis Common cold Acute laryngitis Otitis externa Mastoiditis Acute apiglottis
Human Influenza. Dr. Sina Soleimani. Human Viral Vaccine Quality Control 89/2/29. November 2, 2011 HVVQC ١
 Human Influenza Dr. Sina Soleimani Human Viral Vaccine Quality Control 89/2/29 November 2, 2011 HVVQC ١ Presentation outline 1. Introduction 2. Virology 3. Classification 4. Hosts 5. Antigenic Specifications
Human Influenza Dr. Sina Soleimani Human Viral Vaccine Quality Control 89/2/29 November 2, 2011 HVVQC ١ Presentation outline 1. Introduction 2. Virology 3. Classification 4. Hosts 5. Antigenic Specifications
Respiratory tract infections. Krzysztof Buczkowski
 Respiratory tract infections Krzysztof Buczkowski Etiology Viruses Rhinoviruses Adenoviruses Coronaviruses Influenza and Parainfluenza Viruses Respiratory Syncitial Viruses Enteroviruses Etiology Bacteria
Respiratory tract infections Krzysztof Buczkowski Etiology Viruses Rhinoviruses Adenoviruses Coronaviruses Influenza and Parainfluenza Viruses Respiratory Syncitial Viruses Enteroviruses Etiology Bacteria
Human infection with pandemic (H1N1) 2009 virus: updated interim WHO guidance on global surveillance
 2009 virus: updated interim WHO guidance on global surveillance") Human infection with pandemic (H1N1) 2009 virus: updated interim WHO guidance on global surveillance 10 July 2009 Background This document updates the interim WHO guidance on global surveillance of pandemic
Human infection with pandemic (H1N1) 2009 virus: updated interim WHO guidance on global surveillance 10 July 2009 Background This document updates the interim WHO guidance on global surveillance of pandemic
4/7/13 SINUSITIS WHO ARE WE TREATING? AMANDA SAM CONLEY RN, MSN, CFN, LNC, FNP- BC
 SINUSITIS WHO ARE WE TREATING? AMANDA SAM CONLEY RN, MSN, CFN, LNC, FNP- BC 1 DefiniGons Anatomy Review Signs and Symptoms OBJECTIVES Acute Viral vrs. Acute Bacterial Treatment Guidelines ANATOMY REVIEW
SINUSITIS WHO ARE WE TREATING? AMANDA SAM CONLEY RN, MSN, CFN, LNC, FNP- BC 1 DefiniGons Anatomy Review Signs and Symptoms OBJECTIVES Acute Viral vrs. Acute Bacterial Treatment Guidelines ANATOMY REVIEW
INFLUENZA AND OTHER RESPIRATORY VIRUSES
 INFLUENZA AND OTHER RESPIRATORY VIRUSES Lung Foundation Australia Patient Seminar 21 st October 2017 Lynette Reid Respiratory Clinical Nurse Specialist, RHH What is influenza (the flu )? Influenza (flu)
INFLUENZA AND OTHER RESPIRATORY VIRUSES Lung Foundation Australia Patient Seminar 21 st October 2017 Lynette Reid Respiratory Clinical Nurse Specialist, RHH What is influenza (the flu )? Influenza (flu)
NOVEL INFLUENZA A (H1N1) Swine Flu
 Swine Flu") Introduction Definitions Influenza-like Illness Emergency Department Assessment Anitiviral Medication Oseltamivir (Tamiflu) Dosing Infection Control Issues Staff Exposure References Introduction This guideline
Introduction Definitions Influenza-like Illness Emergency Department Assessment Anitiviral Medication Oseltamivir (Tamiflu) Dosing Infection Control Issues Staff Exposure References Introduction This guideline
What is Influenza? Patricia Daly MD, FRCPC Medical Health Officer and Medical Director of Communicable Disease Control
 Vancouver Coastal Health & The Vancouver Coastal Health Research Institute presents: On Call with VGH Experts Lecture Series The Flu and You What is Influenza? Patricia Daly MD, FRCPC Medical Health Officer
Vancouver Coastal Health & The Vancouver Coastal Health Research Institute presents: On Call with VGH Experts Lecture Series The Flu and You What is Influenza? Patricia Daly MD, FRCPC Medical Health Officer
STANDING ORDERS FOR ANTIVIRAL THERAPY AND POST-ExPOSURE PROPHYLAXIS TO INFLUENZA A AND B: OSELTAMIVIR, RIMANTADINE, AND ZANAMIVIR
 STANDING ORDERS FOR ANTIVIRAL THERAPY AND POST-ExPOSURE PROPHYLAXIS TO INFLUENZA A AND B: OSELTAMIVIR, RIMANTADINE, AND ZANAMIVIR Purpose: To reduce the morbidity and mortality from influenza infection
STANDING ORDERS FOR ANTIVIRAL THERAPY AND POST-ExPOSURE PROPHYLAXIS TO INFLUENZA A AND B: OSELTAMIVIR, RIMANTADINE, AND ZANAMIVIR Purpose: To reduce the morbidity and mortality from influenza infection
INFLUENZA (Outbreaks; hospitalized or fatal pediatric cases)
") INFLUENZA (Outbreaks; hospitalized or fatal pediatric cases) 1. Agent: Influenza viruses A, B, and C. Only influenza A and B are of public health concern since they are responsible for epidemics. 2. Identification:
INFLUENZA (Outbreaks; hospitalized or fatal pediatric cases) 1. Agent: Influenza viruses A, B, and C. Only influenza A and B are of public health concern since they are responsible for epidemics. 2. Identification:
Antivirals for Avian Influenza Outbreaks
 Antivirals for Avian Influenza Outbreaks Issues in Influenza Pandemic Preparedness 1. Surveillance for pandemic preparedness eg. H5N1 2. Public health intervention eg. efficacy, feasibility and impact
Antivirals for Avian Influenza Outbreaks Issues in Influenza Pandemic Preparedness 1. Surveillance for pandemic preparedness eg. H5N1 2. Public health intervention eg. efficacy, feasibility and impact
The Flu December 2017
 1 Ohio Northern University - HealthWise The Flu December 2017 Protect Yourself From The Flu! Flu Health Flu season is upon us! Are you ready? This newsletter will provide information to help protect yourself
1 Ohio Northern University - HealthWise The Flu December 2017 Protect Yourself From The Flu! Flu Health Flu season is upon us! Are you ready? This newsletter will provide information to help protect yourself
INFLUENZA WHAT YOU NEED TO KNOW ARE YOU SURE YOU USE THE RIGHT MEASURES TO PROTECT YOURSELF AGAINST THE FLU?
 INFLUENZA WHAT YOU NEED TO KNOW ARE YOU SURE YOU USE THE RIGHT MEASURES TO PROTECT YOURSELF AGAINST THE FLU? GET INFORMED! GET VACCINATED! GET PROTECTED! FLU VACCINE WHAT IS INFLUENZA? Seasonal influenza
INFLUENZA WHAT YOU NEED TO KNOW ARE YOU SURE YOU USE THE RIGHT MEASURES TO PROTECT YOURSELF AGAINST THE FLU? GET INFORMED! GET VACCINATED! GET PROTECTED! FLU VACCINE WHAT IS INFLUENZA? Seasonal influenza
SINUSITIS. HAVAS ENT CLINICS Excellence in otolaryngology
 JULY 2015 SINUSITIS WHAT IS IT? WHAT SHOULD YOU DO? WHAT WORKS? THOMAS E HAVAS MBBS (SYD) MD (UNSW) FRCSE, FRACS, FACS CONJOINT ASSOCIATE PROFESSOR UNSW OTOLARNGOLOGY HEAD AND NECK SURGERY HAVAS ENT CLINICS
JULY 2015 SINUSITIS WHAT IS IT? WHAT SHOULD YOU DO? WHAT WORKS? THOMAS E HAVAS MBBS (SYD) MD (UNSW) FRCSE, FRACS, FACS CONJOINT ASSOCIATE PROFESSOR UNSW OTOLARNGOLOGY HEAD AND NECK SURGERY HAVAS ENT CLINICS
Diagnosis and Treatment of Respiratory Illness in Children and Adults Guideline
 Member Groups Requesting Changes: Lakeview Clinic Marshfield Clinic Mayo Clinic South Lake Pediatrics Response Report for Review and Comment January 2013 Diagnosis and Treatment of Respiratory Illness
Member Groups Requesting Changes: Lakeview Clinic Marshfield Clinic Mayo Clinic South Lake Pediatrics Response Report for Review and Comment January 2013 Diagnosis and Treatment of Respiratory Illness
WHO Technical Consultation on the severity of disease caused by the new influenza A (H1N1) virus infections
 virus infections") WHO Technical Consultation on the severity of disease caused by the new influenza A (H1N1) virus infections Original short summary posted 6 May 2009. Revised full report posted May 9 2009. On 5 May 2009
WHO Technical Consultation on the severity of disease caused by the new influenza A (H1N1) virus infections Original short summary posted 6 May 2009. Revised full report posted May 9 2009. On 5 May 2009
Influenza Backgrounder
 Influenza Backgrounder Influenza Overview Influenza causes an average of 36,000 deaths and 200,000 hospitalizations in the U.S. every year. 1,2 Combined with pneumonia, influenza is the seventh leading
Influenza Backgrounder Influenza Overview Influenza causes an average of 36,000 deaths and 200,000 hospitalizations in the U.S. every year. 1,2 Combined with pneumonia, influenza is the seventh leading
Influenza. Tim Uyeki MD, MPH, MPP, FAAP
 Influenza Tim Uyeki MD, MPH, MPP, FAAP Influenza Division National Center for Immunization and Respiratory Diseases Coordinating Center for Infectious Diseases Centers for Disease Control and Prevention
Influenza Tim Uyeki MD, MPH, MPP, FAAP Influenza Division National Center for Immunization and Respiratory Diseases Coordinating Center for Infectious Diseases Centers for Disease Control and Prevention
Guideline Summary NGC-5582
 Guideline Summary NGC-5582 Guideline Title Antiviral therapy and prophylaxis for influenza in children. Bibliographic Source(s) American Academy of Pediatrics Committee on Infectious Diseases. Antiviral
Guideline Summary NGC-5582 Guideline Title Antiviral therapy and prophylaxis for influenza in children. Bibliographic Source(s) American Academy of Pediatrics Committee on Infectious Diseases. Antiviral
دکتر بهروز نقیلی استاد بیماریهای عفونی مرکس تحقیقات بیماریهای عفونی و گرمسیری پاییس 88
 دکتر بهروز نقیلی استاد بیماریهای عفونی مرکس تحقیقات بیماریهای عفونی و گرمسیری پاییس 88 FLU.. How often can you escape? Three viral types are distinguished by their matrix and nucleoproteins Type Host Clinical
دکتر بهروز نقیلی استاد بیماریهای عفونی مرکس تحقیقات بیماریهای عفونی و گرمسیری پاییس 88 FLU.. How often can you escape? Three viral types are distinguished by their matrix and nucleoproteins Type Host Clinical
Influenza Therapies. Considerations Prescription influenza therapies require prior authorization through pharmacy services.
 Influenza Therapies Policy Number: 5.01.515 Last Review: 10/2017 Origination: 10/2002 Next Review: 10/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for influenza
Influenza Therapies Policy Number: 5.01.515 Last Review: 10/2017 Origination: 10/2002 Next Review: 10/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for influenza
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Jain S, Kamimoto L, Bramley AM, et al. Hospitalized patients
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Jain S, Kamimoto L, Bramley AM, et al. Hospitalized patients
Swine flu - information prescription
 Swine flu - information prescription Introduction Swine flu is a relatively new strain of influenza (flu) that was responsible for a flu pandemic during 2009-2010. It is sometimes known as H1N1 influenza
Swine flu - information prescription Introduction Swine flu is a relatively new strain of influenza (flu) that was responsible for a flu pandemic during 2009-2010. It is sometimes known as H1N1 influenza
H1N1 Influenza. Influenza-A Basics. Influenza Basics. April 1, History of Influenza Pandemics. April 1 September 25, 2009
 April 1, 2009 H1N1 Influenza Jeff Goad, Pharm.D., MPH Associate Professor of Clinical Pharmacy USC School of Pharmacy April 1 September 25, 2009 History of Influenza Pandemics 400 B.C. 1889 Russian Flu
April 1, 2009 H1N1 Influenza Jeff Goad, Pharm.D., MPH Associate Professor of Clinical Pharmacy USC School of Pharmacy April 1 September 25, 2009 History of Influenza Pandemics 400 B.C. 1889 Russian Flu
Community Acquired Pneumonia
 April 2014 References: 1. Bradley JS, Byington CL, Shah SS, Alverson B, Carter ER, Harrison C, Kaplan SL Mace SE, McCracken Jr. GH, Moor MR, St. Peter SD, Stockwell JA, and Swanson JT. The Management of
April 2014 References: 1. Bradley JS, Byington CL, Shah SS, Alverson B, Carter ER, Harrison C, Kaplan SL Mace SE, McCracken Jr. GH, Moor MR, St. Peter SD, Stockwell JA, and Swanson JT. The Management of
colds and flu Introduction KEY MESSAGES
 colds and flu New insights: Cold and flu Introduction Colds and flu are responsible for more visits to the pharmacy than any other infectious illness. While severity of influenza differs from year to year,
colds and flu New insights: Cold and flu Introduction Colds and flu are responsible for more visits to the pharmacy than any other infectious illness. While severity of influenza differs from year to year,
Diagnosis and Treatment of Respiratory Illness in Children and Adults
 Page 1 of 9 Main Algorithm Annotations 1. Patient Reports Some Combination of Symptoms Patients may present for an appointment, call into a provider to schedule an appointment or nurse line presenting
Page 1 of 9 Main Algorithm Annotations 1. Patient Reports Some Combination of Symptoms Patients may present for an appointment, call into a provider to schedule an appointment or nurse line presenting
Prophylaxis and Treatment for Influenza among the Elderly
 Respiratory Diseases in the Elderly Prophylaxis and Treatment for Influenza among the Elderly JMAJ 45(6): 245 250, 2002 Hajime GOTO Professor, The First Department of Internal Medicine, Kyorin University
Respiratory Diseases in the Elderly Prophylaxis and Treatment for Influenza among the Elderly JMAJ 45(6): 245 250, 2002 Hajime GOTO Professor, The First Department of Internal Medicine, Kyorin University
Choosing an appropriate antimicrobial agent. 3) the spectrum of potential pathogens
 the spectrum of potential pathogens") Choosing an appropriate antimicrobial agent Consider: 1) the host 2) the site of infection 3) the spectrum of potential pathogens 4) the likelihood that these pathogens are resistant to antimicrobial agents
Choosing an appropriate antimicrobial agent Consider: 1) the host 2) the site of infection 3) the spectrum of potential pathogens 4) the likelihood that these pathogens are resistant to antimicrobial agents
A Winter Free of Cold Understanding the Common Cold and Flu. Camille Aizarani, MD Family Medicine Specialist
 A Winter Free of Cold Understanding the Common Cold and Flu Camille Aizarani, MD Family Medicine Specialist Outline Introduction Is it a cold or flu? The Common Cold Symptoms of Common Cold Tansmission
A Winter Free of Cold Understanding the Common Cold and Flu Camille Aizarani, MD Family Medicine Specialist Outline Introduction Is it a cold or flu? The Common Cold Symptoms of Common Cold Tansmission
Respiratory Infections
 Respiratory Infections NISHANT PRASAD, MD THE DR. JAMES J. RAHAL, JR. DIVISION OF INFECTIOUS DISEASES NEWYORK-PRESBYTERIAN QUEENS Disclosures Stockholder: Contrafect Corp., Bristol-Myers Squibb Co Research
Respiratory Infections NISHANT PRASAD, MD THE DR. JAMES J. RAHAL, JR. DIVISION OF INFECTIOUS DISEASES NEWYORK-PRESBYTERIAN QUEENS Disclosures Stockholder: Contrafect Corp., Bristol-Myers Squibb Co Research
INTERNATIONAL SOCIETY FOR HEART AND LUNG TRANSPLANTATION a Society that includes Basic Science, the Failing Heart, and Advanced Lung Disease
 International Society of Heart and Lung Transplantation Advisory Statement on the Implications of Pandemic Influenza for Thoracic Organ Transplantation This advisory statement has been produced by the
International Society of Heart and Lung Transplantation Advisory Statement on the Implications of Pandemic Influenza for Thoracic Organ Transplantation This advisory statement has been produced by the
Structure of viruses
 Antiviral Drugs o Viruses are obligate intracellular parasites. o lack both a cell wall and a cell membrane. o They do not carry out metabolic processes. o Viruses use much of the host s metabolic machinery.
Antiviral Drugs o Viruses are obligate intracellular parasites. o lack both a cell wall and a cell membrane. o They do not carry out metabolic processes. o Viruses use much of the host s metabolic machinery.
Viral Infections of the Respiratory System. Dr. MONA BADR Assistant Professor College of Medicine & KKUH
 Viral Infections of the Respiratory System Dr. MONA BADR Assistant Professor College of Medicine & KKUH Objectives Introduction to respiratory viral infections Characteristics of respiratory viruses (Orthomyxoviridae,
Viral Infections of the Respiratory System Dr. MONA BADR Assistant Professor College of Medicine & KKUH Objectives Introduction to respiratory viral infections Characteristics of respiratory viruses (Orthomyxoviridae,
ORTHOMYXOVIRUSES INFLUENZA VIRUSES. (A,B and C)
") ORTHOMYXOVIRUSES INFLUENZA VIRUSES (A,B and C) Orthomyxoviridae Influenza Viruses Epidemiology: Influenza A virus is so subjected to major antigenic changes that cause occasional world wide pandemics when
ORTHOMYXOVIRUSES INFLUENZA VIRUSES (A,B and C) Orthomyxoviridae Influenza Viruses Epidemiology: Influenza A virus is so subjected to major antigenic changes that cause occasional world wide pandemics when
Influenza 2009: Not Yet The Perfect Storm
 Influenza 2009: Not Yet The Perfect Storm What s needed for a pandemic strain? Novel virus (little to no immunity) Capable of causing disease in humans Highly pathogenic / virulent Capable of sustained
Influenza 2009: Not Yet The Perfect Storm What s needed for a pandemic strain? Novel virus (little to no immunity) Capable of causing disease in humans Highly pathogenic / virulent Capable of sustained
Ralph KY Lee Honorary Secretary HKIOEH
 HKIOEH Round Table: Updates on Human Swine Influenza Facts and Strategies on Disease Control & Prevention in Occupational Hygiene Perspectives 9 July 2009 Ralph KY Lee Honorary Secretary HKIOEH 1 Influenza
HKIOEH Round Table: Updates on Human Swine Influenza Facts and Strategies on Disease Control & Prevention in Occupational Hygiene Perspectives 9 July 2009 Ralph KY Lee Honorary Secretary HKIOEH 1 Influenza
Running head: INFLUENZA VIRUS SEASON PREPAREDNESS AND RESPONSE 1
 Running head: INFLUENZA VIRUS SEASON PREPAREDNESS AND RESPONSE 1 Electron micrograph of H1N1 Virus (CDC, 2009) Influenza Virus Season Preparedness and Response Patricia Bolivar Walden University Epidemiology
Running head: INFLUENZA VIRUS SEASON PREPAREDNESS AND RESPONSE 1 Electron micrograph of H1N1 Virus (CDC, 2009) Influenza Virus Season Preparedness and Response Patricia Bolivar Walden University Epidemiology
Influenza: Seasonal, Avian, and Otherwise
 Influenza: Seasonal, Avian, and Otherwise Lisa Winston, MD University of California, San Francisco San Francisco General Hospital Influenza biology Antiviral medications Seasonal influenza Vaccination
Influenza: Seasonal, Avian, and Otherwise Lisa Winston, MD University of California, San Francisco San Francisco General Hospital Influenza biology Antiviral medications Seasonal influenza Vaccination
Influenza Infection In Human. Dr. Zuhaida A. Jalil Surveillance Sector Disease Control Division, MOH Malaysia 3 May 2018
 Influenza Infection In Human Dr. Zuhaida A. Jalil Surveillance Sector Disease Control Division, MOH Malaysia 3 May 2018 Objective of the session: After completing this session, you will be able to: Understand
Influenza Infection In Human Dr. Zuhaida A. Jalil Surveillance Sector Disease Control Division, MOH Malaysia 3 May 2018 Objective of the session: After completing this session, you will be able to: Understand
Seasonal Influenza Report
 Key findings for the 2017 2018 flu season October 1 st, 2017 (CDC Disease Week 40) marked the beginning of the 2017 2018 influenza season. Influenza activity is increasing in California. As of November
Key findings for the 2017 2018 flu season October 1 st, 2017 (CDC Disease Week 40) marked the beginning of the 2017 2018 influenza season. Influenza activity is increasing in California. As of November
H1N1 Influenza. Situation Update
 TABLE OF CONTENTS H1N1 Influenza 1-2 UIMC Executive Summary of the Management of Novel Influenza A (H1N1) Virus 3-4 Emergency Use of Peramivir Approved 5-6 P&T Committee Formulary Action 6 H1N1 Influenza
TABLE OF CONTENTS H1N1 Influenza 1-2 UIMC Executive Summary of the Management of Novel Influenza A (H1N1) Virus 3-4 Emergency Use of Peramivir Approved 5-6 P&T Committee Formulary Action 6 H1N1 Influenza
INFLUENZA. Rob Young (James. J. Reid) Faculty of Medicine University of Auckland (Otago)
 Faculty of Medicine University of Auckland (Otago)") INFLUENZA Rob Young (James. J. Reid) Faculty of Medicine University of Auckland (Otago) INFLUENZA Don t confuse with the common cold Symptoms may be similar BUT those with influenza are sick those with
INFLUENZA Rob Young (James. J. Reid) Faculty of Medicine University of Auckland (Otago) INFLUENZA Don t confuse with the common cold Symptoms may be similar BUT those with influenza are sick those with
MANAGEMENT OF RHINOSINUSITIS IN ADOLESCENTS AND ADULTS
 MANAGEMENT OF RHINOSINUSITIS IN ADOLESCENTS AND ADULTS Ministry of Health Malaysia Malaysian Society of Otorhinolaryngologist - Head & Neck Surgeons (MS)-HNS) Academy of Medicine Malaysia KEY MESSAGES
MANAGEMENT OF RHINOSINUSITIS IN ADOLESCENTS AND ADULTS Ministry of Health Malaysia Malaysian Society of Otorhinolaryngologist - Head & Neck Surgeons (MS)-HNS) Academy of Medicine Malaysia KEY MESSAGES
Seasonal Influenza Report
 Key findings for the 2017 2018 flu season Seasonal Influenza Report 2017 2018 Influenza activity is widely circulating in California. As of week 52 (December 24 30, 2017), the statewide geographic distribution
Key findings for the 2017 2018 flu season Seasonal Influenza Report 2017 2018 Influenza activity is widely circulating in California. As of week 52 (December 24 30, 2017), the statewide geographic distribution
Drugs Used to Treat Chronic Obstructive Pulmonary Disease (COPD)
") Drugs Used to Treat Chronic Obstructive Pulmonary Disease (COPD) COPD COPD is a chronic, irreversible obstruction of airflow that is usually progressive. Symptoms include cough, excess mucus production,
Drugs Used to Treat Chronic Obstructive Pulmonary Disease (COPD) COPD COPD is a chronic, irreversible obstruction of airflow that is usually progressive. Symptoms include cough, excess mucus production,